|
Overview
 There are three types of flat feet: flexible flatfoot, painful rigid flatfoot, and spasmodic flatfoot. Flexible flat feet have some arch, even if the arch only appears while the person is flexing the foot or standing on their toes. Flexible flat feet may not cause pain or require treatment. Painful rigid flatfoot, on the other hand, is abnormal and causes pain, stiffness, and the inability to flex the foot. This often indicates that there is a problem with the bones in the foot, a disease is present, or an injury has occurred. Spasmodic flatfoot involves the foot being forced outward by spasmodic contractions of the peroneal muscle. Causes Most commonly fallen arches in adulthood can arise due to Posterior Tibial Tendon Dysfunction (PTTD). The posterior tibial tendon plays a pivotal role in holding up the arch of the foot, damage to this tendon results in the arch collapsing. Another cause of acquired flat feet in adulthood may be due to Rheumatoid arthritis as this disease attacks the bone, cartilage and ligaments in the foot causing it to change shape and flatten. Injury to the ligament, fracture and/or dislocation of the bones in the mid foot can all lead to a flat foot deformity. Adult acquired flat fleet can also arise in people who have diabetes or a neurological condition which limits normal feeling in the foot, the muscles in feet switch off, the tendons and ligaments weaken, and the arch eventually collapses. Symptoms It?s possible to have fallen arches and experience no symptoms whatsoever. But many people do notice some problems with this condition. Their feet, back and legs ache. Standing on their toes is difficult, if not impossible, and they note swelling around the arch and heel. Diagnosis Podiatrists are trained in expertly assessing flat feet and identifying different risk factors and the causes for it. Initial assessment will begin with a detailed history attempting to find out if any underlying illness has resulted in this. A detailed clinical examination normally follows. The patient may be asked to perform certain movements such as walking or standing on their toes to assess the function of the foot. Footwear will also be analysed to see if there has been excessive wear or if they are contributing to the pronation of the foot. To assess the structure of the foot further, the podiatrist may perform certain x-rays to get a detailed idea of the way the bones are arranged and how the muscle tissues may be affecting them. It also helps assess any potential birth defects in a bit more detail. fallen arches surgery Non Surgical Treatment If your condition is bothersome, try elevating your feet and using ice on the arches to reduce swelling. Your podiatrist can recommend several orthotic aids and inserts to strengthen the tendons of your foot. He can also demonstrate stretching exercises or refer you to physical therapy to get those tendons back into shape. If the symptoms of fallen arches are painful and troubling, he may recommend a steroid injection to relieve inflammation and pain. And in some instances, he may determine that surgery is necessary. Surgical Treatment  Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Stage one deformities usually respond to conservative or non-surgical therapy such as anti-inflammatory medication, casting, functional orthotics or a foot ankle orthosis called a Richie Brace. If these modalities are unsuccessful surgery is warranted. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss. Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint. After Care Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low. Overview
Surgery to shorten the longer leg. This is less involved than lengthening the shorter leg. Shortening may be done in one of two ways. Closing the growth plate of the long leg 2-3 years before growth ends (around age 11-13), letting the short leg catch up. This procedure is called an epiphysiodesis. Taking some bone from the longer leg once growth is complete to even out leg lengths. Surgery to lengthen the shorter leg. This surgery is more involved than surgery to shorten a leg. During this surgery, cuts are made in the leg bone. An external metal frame and bar are attached to the leg bone. This frame and bar slowly pull on the leg bone, lengthening it. The frame and bar must be worn constantly for months to years. When the frame and bar are removed, a leg cast is required for several months. This surgery requires careful and continued follow-up with the surgeon to be sure that healing is going well.  Causes Leg length discrepancies can be caused by: hip and knee replacements, lower limb injuries, bone diseases, neuromuscular issues and congenital problems. Although discrepancies of 2 cm or less are most common, discrepancies can be greater than 6 cm. People who have LLD tend to make up for the difference by over bending their longer leg or standing on the toes of their shorter leg. This compensation leads to an inefficient, up and down gait, which is quite tiring and over time can result in posture problems as well as pain in the back, hips, knees and ankles. Symptoms Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions. Diagnosis Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement. Non Surgical Treatment Treatment of leg length inequality involves many different approaches, such as orthotics, epiphysiodesis, shortening, and lengthening, which can be used alone or combined in an effort to achieve equalization of leg lengths. Leg length inequality of 2 cm or less is usually not a functional problem. Often, leg length can be equalized with a shoe lift, which usually corrects about two thirds of the leg length inequality. Up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear. Leg length inequalities beyond 5 cm are difficult to treat with a shoe lift. The shoe looks unsightly, and often the patient complains of instability with such a large lift. A foot-in-foot prosthesis can be used for larger leg length inequalities. This is often done as a temporizing measure for young children with significant leg length inequalities. The prosthesis is bulky, and a fixed equinus contracture may result.  how to increase height naturally after 18 Surgical Treatment In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened. Overview
Differences between the lengths of the upper and/or lower legs are called leg length discrepancies (LLD). A leg length difference may simply be a mild variation between the two sides of the body. This is not unusual in the general population. For example, one study reported that 32 percent of 600 military recruits had a 1/5 inch to a 3/5 inch difference between the lengths of their legs. This is a normal variation. Greater differences may need treatment because a significant difference can affect a patient's well-being and quality of life.  Causes A patient?s legs may be different lengths for a number of reasons, including a broken leg bone may heal in a shorter position, particularly if the injury was severe. In children, broken bones may grow faster for a few years after they heal, resulting in one longer leg. If the break was near the growth center, slower growth may ensue. Children, especially infants, who have a bone infection during a growth spurt may have a greater discrepancy. Inflammation of joints, such as juvenile arthritis during growth, may cause unequal leg length. Compensation for spinal or pelvic scoliosis. Bone diseases such as Ollier disease, neurofibromatosis, or multiple hereditary exostoses. Congenital differences. Symptoms LLD do not have any pain or discomfort directly associated with the difference of one leg over the other leg. However, LLD will place stress on joints throughout the skeletal structure of the body and create discomfort as a byproduct of the LLD. Just as it is normal for your feet to vary slightly in size, a mild difference in leg length is normal, too. A more pronounced LLD, however, can create abnormalities when walking or running and adversely affect healthy balance and posture. Symptoms include a slight limp. Walking can even become stressful, requiring more effort and energy. Sometimes knee pain, hip pain and lower back pain develop. Foot mechanics are also affected causing a variety of complications in the foot, not the least, over pronating, metatarsalgia, bunions, hammer toes, instep pain, posterior tibial tendonitis, and many more. Diagnosis Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement. Non Surgical Treatment The key to treatment of LLD in a child is to predict what the discrepancy is at maturity. If it is predicted to be less than 2 cm., no treatment is needed. Limb length discrepancies of up to 2 or 2.5 cm. can be compensated very well with a lift in the shoe. Beyond 2.5 cm., it becomes increasingly difficult to compensate with a left in the insole. Building up the shoe becomes uncosmetic and cumbersome, and some other way of compensating for the discrepancy becomes necessary. The treatment of LLD is long-term treatment, and involves the physician and patient?s family working together as a team. The family needs to weigh the various options available. If leg lengthening is decided on, the family needs to understand the commitment necessary to see it through. The treatment takes 6 months to a year for completion, and complications can happen. But when it works, the results are gratifying.  what can i do to get taller? Surgical Treatment Surgical lengthening of the shorter extremity (upper or lower) is another treatment option. The bone is lengthened by surgically applying an external fixator to the extremity in the operating room. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins or both. A small crack is made in the bone and tension is created by the frame when it is "distracted" by the patient or family member who turns an affixed dial several times daily. The lengthening process begins approximately five to ten days after surgery. The bone may lengthen one millimeter per day, or approximately one inch per month. Lengthening may be slower in adults overall and in a bone that has been previously injured or undergone prior surgery. Bones in patients with potential blood vessel abnormalities (i.e., cigarette smokers) may also lengthen more slowly. The external fixator is worn until the bone is strong enough to support the patient safely, approximately three months per inch of lengthening. This may vary, however, due to factors such as age, health, smoking, participation in rehabilitation, etc. Risks of this procedure include infection at the site of wires and pins, stiffness of the adjacent joints and slight over or under correction of the bone?s length. Lengthening requires regular follow up visits to the physician?s office, meticulous hygiene of the pins and wires, diligent adjustment of the frame several times daily and rehabilitation as prescribed by your physician. Overview
 Morton's neuroma is a swollen or thickened nerve in the ball of your foot. When your toes are squeezed together too often and for too long, the nerve that runs between your toes can swell and get thicker. This swelling can make it painful when you walk on that foot. High-heeled, tight, or narrow shoes can make pain worse. Sometimes, changing to shoes that give your toes more room can help. Morton's neuroma is a swollen or thickened nerve in the ball of your foot. When your toes are squeezed together too often and for too long, the nerve that runs between your toes can swell and get thicker. This swelling can make it painful when you walk on that foot. High-heeled, tight, or narrow shoes can make pain worse. Sometimes, changing to shoes that give your toes more room can help.Causes Pronation of the foot can cause the metatarsal heads to rotate slightly and pinch the nerve running between the metatarsal heads. This chronic pinching can make the nerve sheath enlarge. As it enlarges it than becomes more squeezed and increasingly troublesome. Tight shoes, shoes with little room for the forefoot, pointy toeboxes can all make this problem more painful. Walking barefoot may also be painful, since the foot may be functioning in an over-pronated position. Symptoms The symptoms of a Morton's neuroma are classic in nature. The patient complains of a burning , tingling, slightly numb feeling (dysesthesias) which radiates out to the toes on either side of the interspace that is involved. For instance, a Morton's neuroma of the third interspace will result in pain between the third and fourth toes, and a neuroma in the second interspace will cause pain between the second and third toes. The symptoms are usually aggravated by wearing shoes, particularly those with high heels. Symptoms are relieved by walking in flat, wide shoes or going barefoot. Rarely will the patient experience pain when sitting or laying down. Diagnosis Morton?s neuroma can be identified during a physical exam, after pressing on the bottom of the foot. This maneuver usually reproduces the patient?s pain. MRI and ultrasound are imaging studiesthat can demonstrate the presence of the neuroma. An x-ray may also be ordered to make sure no other issues exist in the foot. A local anesthetic injection along the neuroma may temporarily abolish the pain, and help confirm the diagnosis. Non Surgical Treatment Rest. Continuing with normal training will increase pain and inflammation and prevent the injury from healing. Wear a metatarsal pad under the forefoot which will raise and spread the bones of the forefoot taking the pressure off the nerve. Wearing metatarsal pads in the shoes under the forefoot spreads the metatarsals creating more space for the nerve. See a sports injury professional who can advise on treatment and rehabilitation. Orthotic inserts may be required to correct any biomechanical dysfunction of the foot. 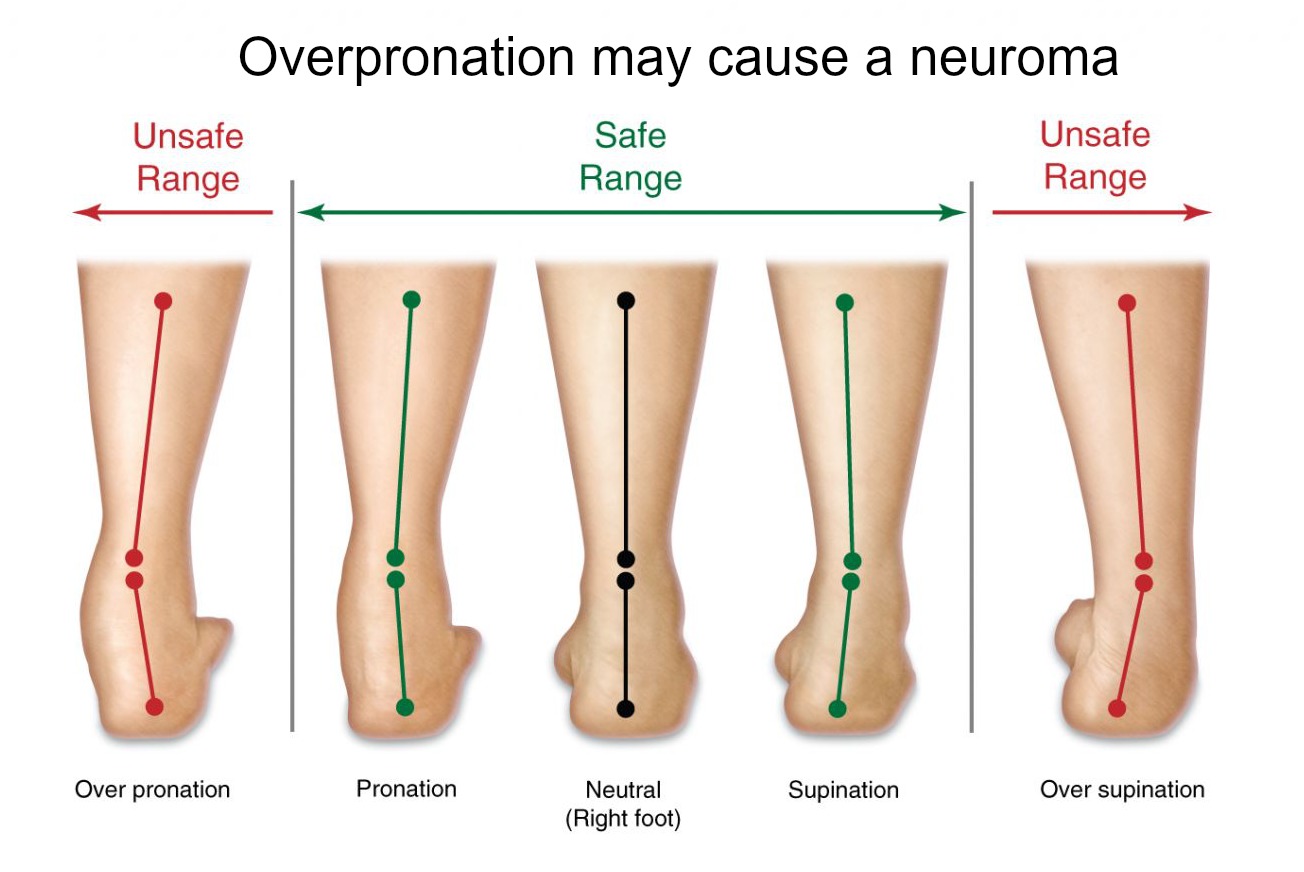 Surgical Treatment The ultimate success of a Morton?s neuroma treated surgically can be variable. In cases where the underlying problem is only an irritated nerve (a true Morton?s neuroma), then surgery will probably be curative (although it may take a few months for the foot to fully heal). But in many cases, forefoot pain is more complex. There may be an irritated nerve or two causing pain, but the real problem is often excessive loading of the lesser metatarsals. The generic term for this condition is metatarsalgia. When considering surgery, identifying and addressing these problems may lead to a better end result. There are actually two different types of leg length discrepancies, congenital and acquired. Congenital indicates you are born with it. One leg is anatomically shorter than the other. As a result of developmental phases of aging, the brain senses the gait pattern and identifies some difference. Your body typically adapts by dipping one shoulder to the "short" side. A difference of under a quarter inch isn't really abnormal, does not need Shoe Lifts to compensate and normally doesn't have a serious effect over a lifetime.
 Leg length inequality goes largely undiagnosed on a daily basis, yet this condition is simply fixed, and can eradicate numerous incidents of back problems. Treatment for leg length inequality typically consists of Shoe Lifts. Many are low-priced, often being less than twenty dollars, in comparison to a custom orthotic of $200 or higher. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe. Lumbar pain is the most widespread condition afflicting people today. Over 80 million people suffer from back pain at some point in their life. It's a problem that costs businesses huge amounts of money each year because of lost time and production. Innovative and improved treatment methods are continually sought after in the hope of decreasing the economic influence this issue causes.  Men and women from all corners of the world experience foot ache due to leg length discrepancy. In most of these situations Shoe Lifts might be of immense help. The lifts are capable of relieving any pain in the feet. Shoe Lifts are recommended by numerous experienced orthopaedic practitioners". So that you can support the human body in a well balanced fashion, feet have got a critical part to play. Inspite of that, it is often the most neglected region of the body. Many people have flat-feet which means there is unequal force placed on the feet. This causes other parts of the body including knees, ankles and backs to be affected too. Shoe Lifts guarantee that suitable posture and balance are restored.  Overview OverviewA Hammer toe is a deformity of the second, third or fourth toe in which the toe becomes bent at the middle joint; hence, it resembles a hammer. Claw toe and mallet toe are related conditions. While a hammer toe is contracted at the first toe joint, a mallet toe is contracted at the second toe joint, and a claw toe is contracted at both joints. According to the 2012 National Foot Health Assessment conducted by the NPD Group for the Institute for Preventive Foot Health, 3 percent of U.S. adults age 21 and older (about 7 million people) have experienced hammer toe or claw toe. The condition is significantly more prevalent in females than in males. Causes Factors that may increase you risk of hammertoe and mallet toe include age. The risk of hammertoe and mallet toe increases with age. Your sex. Women are much more likely to develop hammertoe or mallet toe than are men. Toe length. If your second toe is longer than your big toe, it's at higher risk of hammertoe or mallet toe.  Symptoms SymptomsSymptoms include sharp pain in the middle of the toe and difficulty straightening the toe. People with hammertoe may also develop blisters, which are fluid-filled pockets of skin, because the bent toe is likely to rub against the inside of a shoe. This increased friction may also lead to calluses, which are areas of thickened skin, and corns, which are hard lumps that may form on or between toes. Symptoms may be minor at first, but they can worsen over time. Diagnosis The earlier a hammertoe is diagnosed, the better the prognosis and treatment options. Your doctor will be able to diagnose your hammertoe with a simple examination of the foot and your footwear. He or she may take an x-ray to check the severity of the condition. You may also be asked about your symptoms, your normal daily activities, and your medical and family history. Non Surgical Treatment The most common treatment is to wear more comfortable shoes. When choosing a shoe, make sure the toe area is high and broad and has enough room for hammer toes. If there is chronic pain, surgery may be needed to correct a malalignment. Surgical treatments are aimed at loosening up the contracted toe joints to allow them to align properly. Other types of treatment are products designed to relieve hammer toes, such as hammer toe crests and hammer toe splints. These devices will help hold down the hammer toe and provide relief to the forefoot. Gel toe shields and gel toe caps can also be used. Gel toe shields and toe caps will help eliminate friction between the shoe and the toe, while providing comfort and lubrication. Surgical Treatment If these treatments are not sufficient at correcting the hammer toe, an operation to straighten the toe may be necessary. This is often performed in conjunction with surgery for a bunion deformity. The surgical treatment of a hammer toe hammertoe can consist of either cutting the tendons to relieve the pressure that causes the deformity, or fusing the toe so that it points straight permanently.  Overview OverviewThe 2nd toe is the most common digit to develop a Hammertoe deformity. Second toe hammer toes commonly result from an elongated 2nd metatarsal and from pressure due to an excessively abducted great toe (hallux valgus deformity) causing a bunion. Unusually long toes often develop hammer toe deformities. Painful corns often develop in hammer toe deformity, particularly of the 5th toe. Reactive adventitial bursas often develop beneath corns, which may become inflamed. Causes The constant pressure a woman's foot receives in high-heeled shoes due to the force of gravity causes their feet to naturally slide down and press on the lowest point of the shoe so they are not able to receive enough space and stretch out. The result is an eventual distortion of the woman's toes. The deformity comes as a result of the shortening of muscles inside the toes because the toes become used to being in a bent position, prompting the muscles to fail to extend any further and become tightened and curbed. At first, toes may still be stretched out if poor footwear is not being worn, yet if the habit is persistent...the person's toes will eventually become used to the position they are constantly in and muscle fibers inside them will harden and refuse to stretch.  Symptoms At first, a hammertoe or mallet toe may maintain its flexibility and lie flat when you're not wearing crowded footwear. But eventually, the tendons of the toe may contract and tighten, causing your toe to become permanently stiff. Your shoes can rub against the raised portion of the toe or toes, causing painful corns or calluses. Diagnosis Your healthcare provider will examine your foot, checking for redness, swelling, corns, and calluses. Your provider will also measure the flexibility of your toes and test how much feeling you have in your toes. You may have blood tests to check for arthritis, diabetes, and infection. Non Surgical Treatment Wear sensible shoes. If you don?t want to have surgery to fix your hammertoe, use non-medicated padding along with proper shoes made with a wider and deeper toe box to accommodate your foot?s shape. Ensuring your shoes have a good arch support can slow the progression of the condition as well. Use a pumice stone. The corn or callus that forms on top of the hammertoe can cause discomfort when you wear shoes. Treat the corn by using a file or pumice stone to reduce its size after a warm bath, then apply emollients to keep the area softened and pliable. Use silicone or moleskin padding on top of the area when wearing shoes. Do foot exercises. Theoretically, exercises like extending, then curling the toes, splaying the toes, and moving the toes individually may help prevent the digital contracture that causes hammertoe. Try these suggestions and see what works best for you. Surgical Treatment In advanced cases in which the toe has become stiff and permanently bent, the toe can be straightened with surgery. One type of surgery involves removing a small section of the toe bone to allow the toe to lie flat. Surgery for hammertoe usually is classified as a cosmetic procedure. Cosmetic foot surgeries sometimes cause complications such as pain or numbness, so it?s better to treat the problem with a shoe that fits properly.
Overview
 A bunion is a bony bump on the joint at the base of your big toe. The bony growth on the joint sometimes causes your big toe to Bunion Surgery at Nuffield Health Hospitalsturn in towards your second toe. Symptoms include pain, swelling of your big toe and, as the bunion sticks out, it can often rub on the inside of your shoe. The cause is not always known, there may be a deformity of the joint, called hallux valgus (hallux means big toe, valgus means bent outwards). Or it can be as simple as ill fitting footwear not allowing enough width to fit the toes in their natural position. Sometimes bunions are associated with arthritis in the joint at the base of your big toe. Left untreated bunions can continue to grow and become more painful. A bunion is a bony bump on the joint at the base of your big toe. The bony growth on the joint sometimes causes your big toe to Bunion Surgery at Nuffield Health Hospitalsturn in towards your second toe. Symptoms include pain, swelling of your big toe and, as the bunion sticks out, it can often rub on the inside of your shoe. The cause is not always known, there may be a deformity of the joint, called hallux valgus (hallux means big toe, valgus means bent outwards). Or it can be as simple as ill fitting footwear not allowing enough width to fit the toes in their natural position. Sometimes bunions are associated with arthritis in the joint at the base of your big toe. Left untreated bunions can continue to grow and become more painful.Causes Bunions have a number of causes, primarily genetics and bad choices in footwear. We inherit traits like flat feet, abnormal bone structure, and loose ligaments and tendons from our parents. When our feet are weakened by these traits and we stuff them into high heels or shoes which don?t support our feet correctly, the repeated stress on the front of the foot may contribute to the formation of a bunion. Other contributing factors are jobs that demand a lot of time standing, obesity, and sudden hormonal changes and weight gain, as in pregnancy. Unfortunately, bunions can lead to many other foot conditions as well. The joint behind the big toe carries much of your body weight and when the bunion makes it sore, you shift your weight onto other areas of the foot. That?s why we frequently see crossover toes, overlapping toes, hammer toes, corns, calluses, and ingrown toenails accompanying bunions. As pain in your foot increases, you?ll also reduce your activity, becoming more sedentary, which has its own quality-of-life issues. Symptoms A bulging bump on the outside of the base of your big toe. Swelling, redness or soreness around your big toe joint aggravated by footwear. Red, calloused skin along the inside edge of the big toe. Corns or calluses under the ball of the foot or where the first and second toes overlap. Persistent or intermittent pain. Restricted movement of your big toe. Diagnosis Looking at the problem area on the foot is the best way to discover a bunion. If it has the shape characteristic of a bunion, this is the first hint of a problem. The doctor may also look at the shape of your leg, ankle, and foot while you are standing, and check the range of motion of your toe and joints by asking you to move your toes in different directions A closer examination with weight-bearing X-rays helps your doctor examine the actual bone structure at the joint and see how severe the problem is. A doctor may ask about the types of shoes you wear, sports or activities (e.g., ballet) you participate in, and whether or not you have had a recent injury. This information will help determine your treatment. Non Surgical Treatment Conservative Treatment. Apply a commercial, nonmedicated bunion pad around the bony prominence. Wear shoes with a wide and deep toe box. If your bunion becomes inflamed and painful, apply ice packs several times a day to reduce swelling. Avoid high-heeled shoes over two inches tall. See your podiatric physician if pain persists. Orthotics. Shoe inserts may be useful in controlling foot function and may reduce symptoms and prevent worsening of the deformity. Padding & Taping. Often the first step in a treatment plan, padding the bunion minimizes pain and allows the patient to continue a normal, active life. Taping helps keep the foot in a normal position, thus reducing stress and pain. Medication. Anti-inflammatory drugs and cortisone injections are often prescribed to ease the acute pain and inflammations caused by joint deformities. Physical Therapy. Often used to provide relief of the inflammation and from bunion pain. Ultrasound therapy is a popular technique for treating bunions and their associated soft tissue involvement.  Surgical Treatment Surgery can be a very successful treatment for bunions and could be considered if you are having pain that is affecting your function on a regular basis, for instance, pain during sports or wearing work shoes. It is important, however, that you are seen by a consultant orthopaedic foot and ankle surgeon who has undergone specialist training with a foot and ankle fellowship. There are many different surgical techniques and it is important that your surgeon is expert in several of these so that you have the one that is best for your unique deformity. Bunion removal is usually done under general anesthesia. This means you will be asleep throughout the procedure. The operation can be performed as a day-case, but an overnight stay in hospital is sometimes required. Your surgeon will explain the benefits and risks of having bunion surgery, and will also discuss the alternatives treatments. Prevention A lot of bunion deformities are hereditary so there isn't much you can do to fully prevent them. Early detection and treatment will go a long way in preventing the growth of the bunion and foot pain. Often times, a good custom orthotic can be very effective in slowing the progression of a bunion, but a podiatrist provides that. Waiting with bunions will worsen the condition and could lead to further complications such as hammertoes or contracted toes. Besides causing deformity, these secondary conditions can eventually cause issues with walking and affect your knees, hip, lower back. There are no lotions over the counter that would be able to actually treat the problem. There are some bunion shields that you can place on the bump to ease symptoms and pressure from shoes. However because this condition is an actual bone deformity, the over the counter option solutions are more like a Band-aid approach. |
